除了 CA199 CA50 胰腺癌的肿瘤标志物 你必须想到它!
众所周知,CA199 和 CA50 作为胰腺癌诊断的生物标志物具有良好的敏感性和特异性。然而,这两种肿瘤标志物都很大程度上受到肝功能和胆汁淤积的影响,从而导致良性胆汁淤积性黄疸和肝实质疾病出现假阳性值。
此外,只有一小部分早期胰腺癌患者能检测到 CA199 和 CA50 水平。在这样的背景下,CA242 「应运而生」!
今天就一起来了解一下肿瘤标志物 CA242:
哪些疾病 CA242 会升高?
诊断胰腺癌,CA242 能否取代 CA199?
CA242 在恶性疾病中的意义?
CA242 是什么?
CA242 是一种唾液酸化的黏蛋白型糖类抗原。1983 年 Lindholm 等人用 COLO205 单克隆抗体免疫小鼠取得了一系列的抗体,1985 年又经过单克隆抗体 CA242 筛选得到了 CA242。
随后他们发现 CA242 在细胞表面以糖蛋白的形式或在血清中以 O-连接的富集糖蛋白形式存在。
哪些疾病 CA242 会升高?
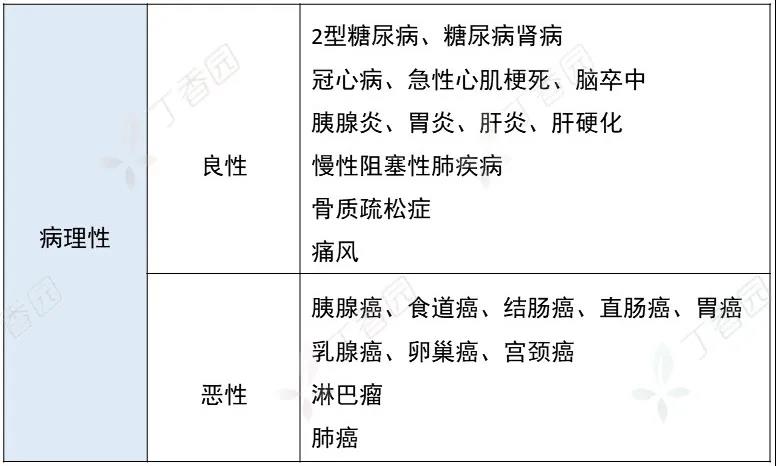
图源:作者
注意:
CA242 在健康人和良性疾病血清中含量很低。正常人体中,仅在结肠的柱状上皮细胞和杯状细胞以及胆管和胰管细胞中有少量的 CA242 表达。
在良性消化系统疾病如胰腺炎、肝炎及肝硬化患者中,CA242 有所升高,但很少升到临界参考值的上界。
CA242 能取代 CA199 吗?
CA242 vs. CEA
CEA 与 CA242 联合检测可提高敏感性,与单独采用 CEA 检测相比,对结肠癌,敏感性可提高 40%-70%;对直肠癌,敏感性提高可达到 47%-62%。CEA 与 CA242 无相关性,具有孤立的诊断价值,且二者之间具有互补性。
CA242 vs. CA199
在胰腺癌的诊断中,CA242 具有与 CA199 和 CA50 相似的敏感性和特异性。
良性疾病尤其是良性肝、胰和胆道疾病,CA19-9 和 CA50 常常会升高,但 CA242 不升高。
尽管在正常组织中或出现胰腺炎时,组织中 CA242 的出现类似于 CA199、CA50,但血清的 CA242 水平并不受胆汁淤积或胆管细胞破坏、胰管狭窄或阻塞等因素影响。
CA242 在恶性疾病中的意义
CA242 与良、恶性肿瘤的鉴别
CA242 主要存在于胰腺和结肠的恶性肿瘤细胞中,它是一种鞘糖脂抗原,不同于 CA199、CA50、CA125 等肿瘤相关抗原,作为肿瘤标志物有更高的特异度,有利于消化道良、恶性肿瘤的鉴别。
CA242 与胰腺癌
辅助诊断
用于胰腺癌的诊断时,CA242 的敏感性可以通过结合癌胚抗原或 CA50 来提高。研究表明,CA242、CA199 和 CA50 对胰腺癌诊断的敏感性分别为 66.2%、70.6% 和 70.6%。CA242 结合 CA50 作为诊断生物标志物,灵敏度可达 75.0%。
判断预后
晚期胰腺癌患者的血清 CA242 水平升高,这表明术前 CA242 的高水平与胰腺癌患者的远处转移情况或预后不良有关。
提示分化程度
IV 期胰腺中高分化癌患者的血清 CA242 水平明显高于低分化癌患者,这表明 CA242 在中高分化癌中的表达明显更强——在分化型肿瘤中比低分化或未分化癌中高。
CA242 作为一种相对较新的胰腺癌生物标记物,有助于胰腺癌治疗的管理,可作为化疗期间疾病进展或手术后复发的临床指标。
参考文献
[1]Lindholm L, Johansson C, Jansson EL, Hallberg C, Nilsson O. An immunoradiometric assay(IRMA) for the CA 50 antigen. In: Holmgren J, ed. Tumour Marker Antigen. Lund,Sweden: Studentlitteratur; 1985:123.
[2]Baeckstrom D, Hansson GC, Nilsson O, Johansson C, Gendler S, Lindholm L. Purification and characterization of a membrane-bound and a secreted mucin-type glycoprotein carrying the carcinoma-associated sialyl-Lea epitope on distinct core proteins. J BiolChem. 1991;266(32):21537–21547.
[3]Kuusela P, Haglund C, Roberts PJ. Comparison of a new tumour marker CA 242 with CA 19-9, CA 50 and carcinoembryonic antigen(CEA) in digestive tract diseases. Br J Cancer. 1991;63(4):636–640.
[4]Banfi G, Zerbi A, Pastori S, Parolini D, Di CV, Bonini P. Behavior of tumor markers CA19.9,CA195, CAM43, CA242, and TPS in the diagnosis and follow-up of pancreatic cancer. Clin Chem. 1993;39(3):420–423.
[5] Röthlin MA, Joller H, Largiadèr F. CA 242 is a new tumor marker for pancreatic cancer. Cancer. 1993 Feb 1;71(3):701-7.
doi: 10.1002/1097-0142(19930201)71:33.0.co;2-c. PMID: 8431849.
[6]Haglund C, Lundin J, Kuusela P, Roberts PJ. CA 242, a new tumour marker for pancreatic cancer: a comparison with CA 19-9, CA 50 and CEA. Br J Cancer.1994;70(3):487–492.
[7]Haglund C, Lindgren J, Roberts PJ, Kuusela P, Nordling S. Tissue expression of the tumour associated antigen CA242 in benign and malignant pancreatic lesions. A comparison with CA 50 and CA 19-9. Br J Cancer. 1989;60(6):845–851.
